Abstract
Objectives
The aim of this study was to introduce a methodology to map irrigant spreadability within the root canal space using micro-computed tomography (micro-CT).
Materials and methods
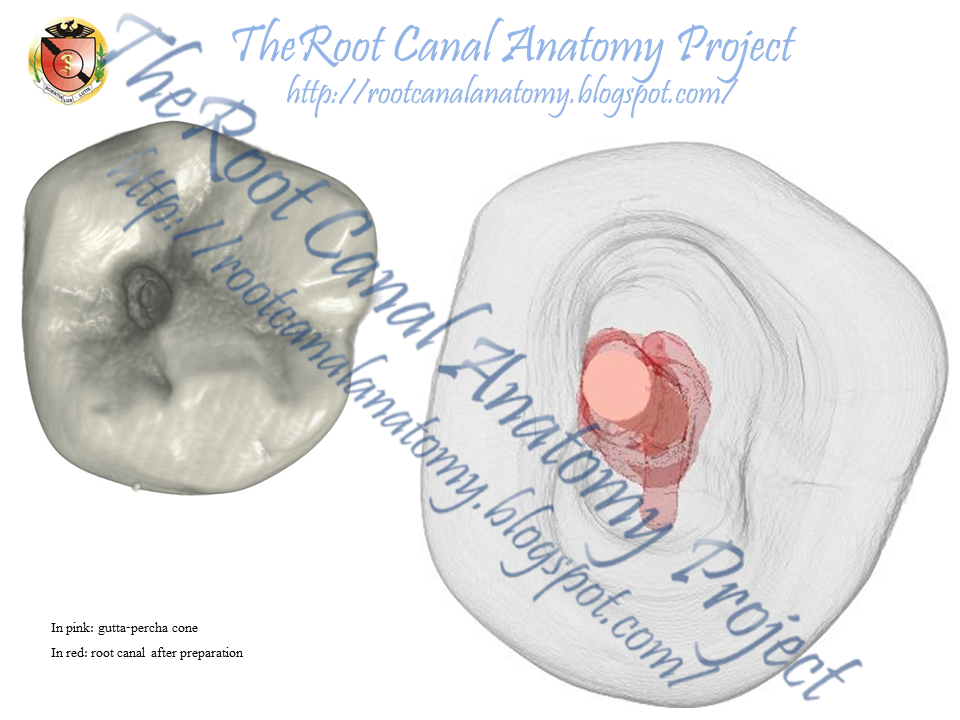
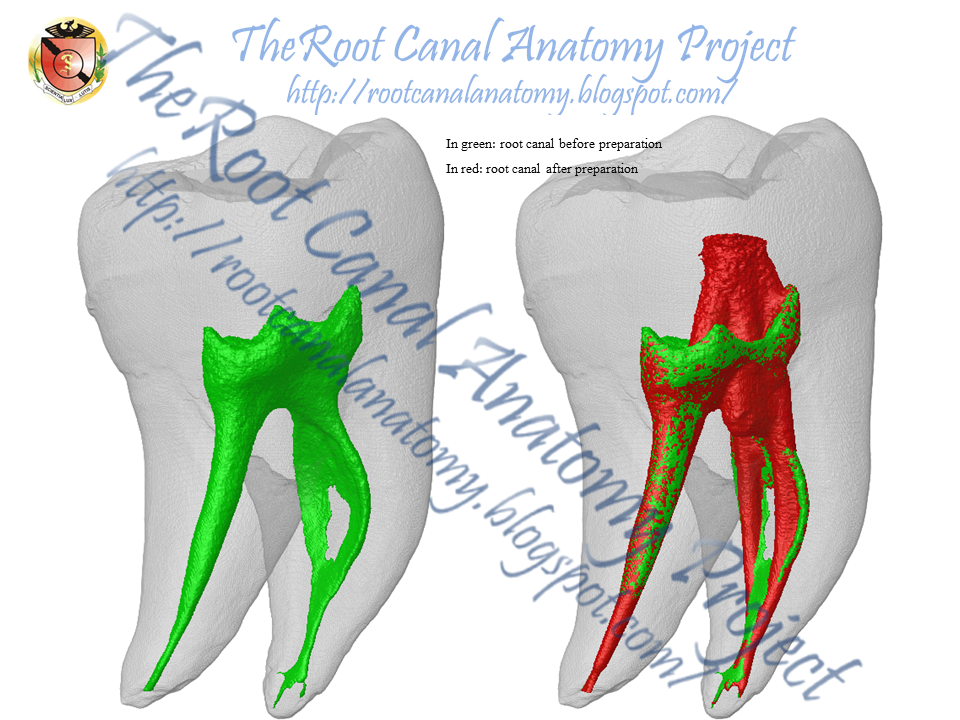
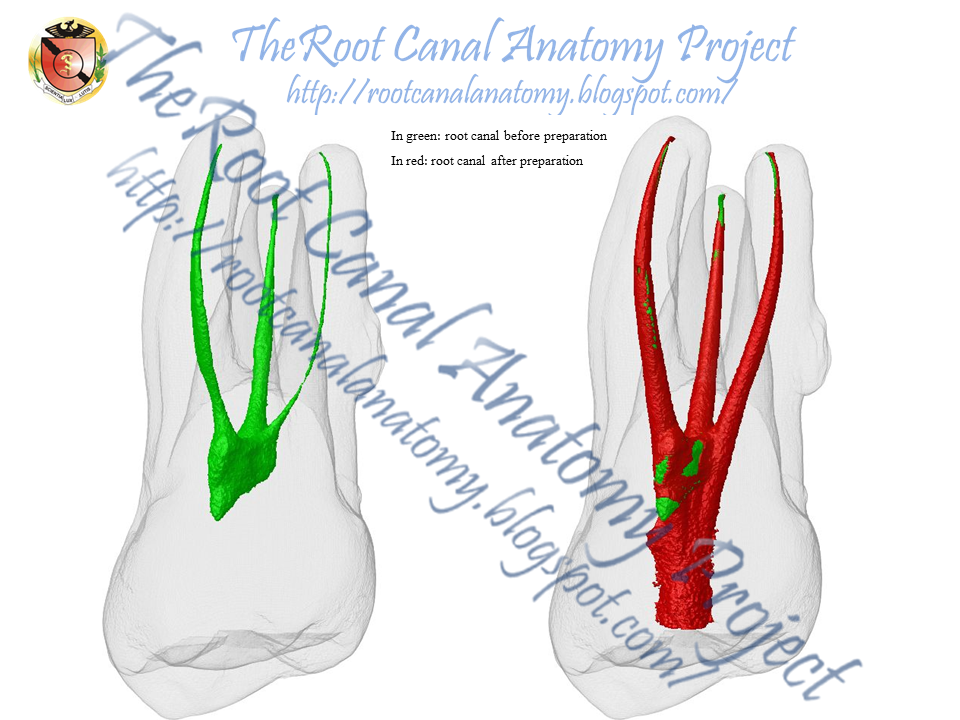
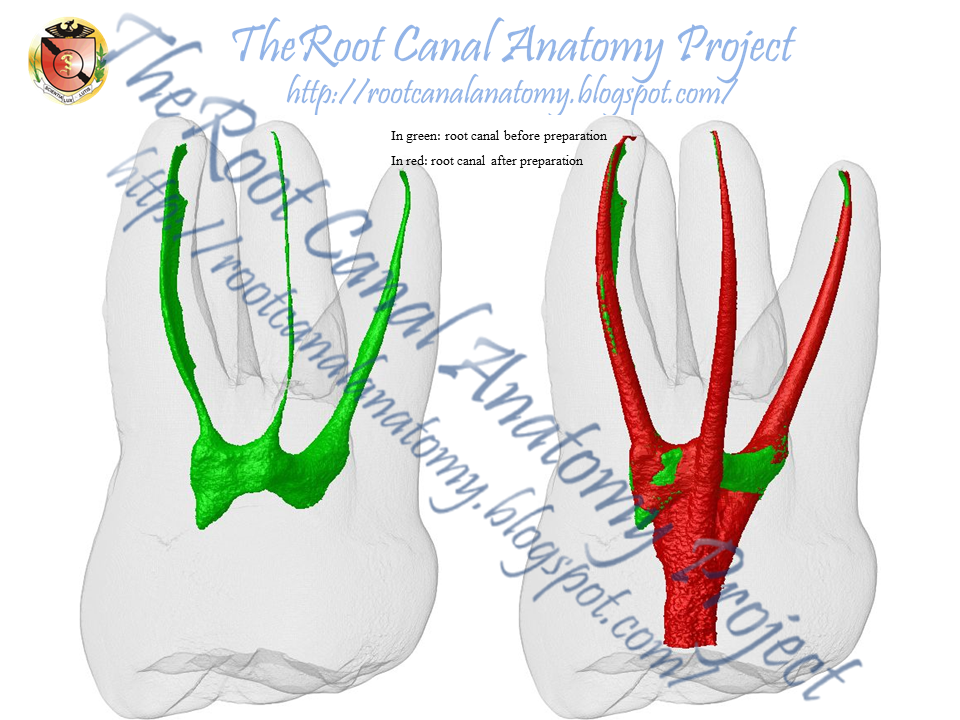
Mandibular molars presenting Vertucci’s types I and II canal configurations were selected, and four scans using isotropic resolution of 19.5 μm were accomplished per tooth: prior to treatment (S1), after glide path (S2) and after root canal preparation (S3 and S4). A contrast solution (CS) was used to irrigate the canals at stages S2 and S4. The touched and untouched surface areas of the canals, the volume of irrigant-free areas and the percentage volume occupied by the CS were calculated. Density, surface tension and the spread pattern of the CS and 2.5 % NaOCl were also evaluated.
Results
In the type I mesial root, there was an increase in the percentage volume of free-irrigated areas from S2 to S4 preparation steps, whilst in the distal roots and type II mesial root, a decrease of irrigant-free areas was observed. The use of CS allowed the quantification of the touched surface area and the volume of the root canal occupied by the irrigating solution. Density (g/mL) and surface tension (mN/m) of the CS and 2.5 % NaOCl were 1.39 and 47.5, and 1.03 and 56.2, respectively. Besides, a similar spread pattern of the CS and 2.5 % NaOCl in a simulated root canal environment was observed.
Conclusions
This study introduced a new methodology for mapping the irrigating solution in the different stages of the root canal preparation and proved useful for in situ volumetric quantification and qualitative evaluation of irrigation spreading and irrigant-free areas.
Clinical relevance
Micro-computed tomographic technology may provide a comprehensive knowledge of the flush effectiveness by different irrigants and delivery systems in order to predict the optimal cleaning and disinfection conditions of the root canal space.